Fundal Height Measurement
How is the measurement of the fundal height related to how far along in gestation you are?
  |
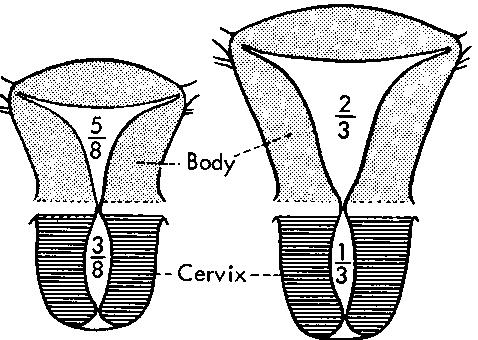 |
If you think of your womb, the uterus, as shaped like a large pear with larger end up, the narrow end is the cervix which crosses the back of the vagina to "empty" into the vagina. In this way, a baby can be stored in the main body of the uterus, the "fundus"--the larger end of the pear shape--and then exit into the outside world through the dilating cervix and via the vagina. The whole path is collectively referred to as the "birth canal," which is a medical slang term.
Before ultrasound, a measurement of the size of the uterus was the most reliable way to document progression of growth (with serial measurements) of the baby; the absolute measurement also gave an indication to how far along the pregnancy was. Of course, one can't measure the entire size of the uterus from examining the abdomen, because some of the uterus lies below the pubic bone, into the pelvis. The best one can do is measure from the pubic bone to the top of the uterus that can be felt. Since all of the growth of the baby is in this part of the uterus anyway (the fundus, or body of the uterus), neglecting the cervix in the measurement isn't a big deal.
How The Measurement Is Done
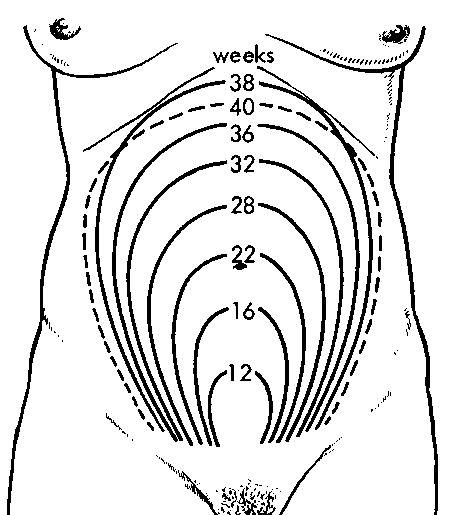
The fundal height--measured from the top of the pubic bone to the top of the uterus--is generally measured in centimeters, and it's a measurement, as you might suspect, that should increase as the pregnancy continues toward your due date. Even though the fundal height is generally a diagnostic tool held over from the days before ultrasound, it is still useful in large clinics where the same patient may not get the same doctor twice in a row for her prenatal visits.
There is no measurement more exact than ultrasound, and even this isn't perfect. But the fundal height, recorded with each visit, is even more inaccurate. Many obstetricians in private practice who see the same patients over and over (small and solo practices), may not even record it, but merely record whether the size of the uterus is compatible with the gestational age. A physician who is familiar with his or her patients will generally know when a baby isn't growing right during the many visits of the pregnancy. And if there is suspicion of a growth restricted baby or an LGA (large for gestational age baby), then ultrasound is the standard of care to sort out any worries--NOT A FUNDAL HEIGHT.
But the fundal height is very useful in the larger clinics, because many different doctors will see a patient before the due date. Because there needs to be at least some objective frame of reference among the different doctors, the fundal height is still a good idea. It's not great, but is easy...and free. Ultrasound would make more academic sense, but is prohibitive from a cost standpoint when attempted on every visit. Like no two scales reading the same weight the same, also no two doctors are going to measure the same fundal height the same. But if a different doctor gets a discrepancy that's wildly different from what was expected based on the previous doctor's fundal height last visit, then ultrasound is justified. This is not very exact science, but it works remarkably well in the larger clinics. Relying on fundal height as above must take into account explainable discrepancies.
- For instance, a baby who has "dropped" between the last visit and the current one may show a fundal height less than last visit! A simple pelvic exam can determine the descent of the baby's head into the maternal pelvis to explain this.
- If a baby's turned sideways, as often occurs in mid-pregnancy, the fundal height can be unusually short for what's expected, because the greatest dimension lies across the horizontal.
- A breech baby, usually sitting up high in the uterus, will yield an unusually large fundal height.
- Twins (or more!) will give a FH way too big for the gestational age. In these days of Assisted Reproductive Technology, this is becoming more common.
These are all circumstances that can defuse concerns over abnormal fundal heights. So it's obvious that it would not be a good idea to revise a due date based on a fundal height.
The fundal height can be out of sync with what's expected for the gestational age due to abnormal conditions:
- Oligohydramnios--too little fluid, taking away from the entire mass effect, leading to a smaller fundal height.
- Hydramnios and polyhydramnios--to much fluid, indicating possibly genetic problems or anatomical problems with the baby.
- Abnormal position of the baby close to term. A sideways baby is forgiveable in midpregnancy, but the later into the pregnancy the unusual position remains, the more likely there could be an abnormality.
The old Charity Hospital trick I use (we used to get people landing there with no prenatal care), is to judge the height of the fundus in relation to the umbilicus (belly button). Generally, the pregnancy is halfway (about 20 weeks) when the fundal height is palpable (felt) at the umbilicus. For every finger's width above the umbilicus the fundal height reaches, you can add a week. Likewise, below the umbilicus, subtracting a week. But this relationship is only applicable between 15 and 25 weeks. Before and after that this relationship goes out the window.
In summary, the fundal height is an antiquated and sometimes obsolete method of judging the appropriate growth of the baby during a pregnancy. It's best use is in large clinics and when a patient presents as a surprise with no prenatal care. But in small private practices, it is superseded by consistent same-physician evaluations throughout the pregnancy.





Share the post with friends: